
This is part of our full report on how digital technology can be incorporated into Local Authority health and wellness services with the aims to save money, work smarter, increase referrals and help more people locally to improve their health. The report is essential reading for public sector professionals working on any form of marketing communications and digital service delivery within local authority teams and service providers. Click here to visit the report home page.
The growth of digital technologies, though by no means universal, is impressive. 92% of the UK population own a mobile phone and 60% use smartphones (forecast to reach 90% by 2020). 58% of C2DE (working class) adults use Facebook and nearly three-quarters of people use the Internet to search about health or medical issues. Source: PHE Marketing Strategy 2014-17
It is clear from our research however that while there are some admirable examples of wellbeing services across the country exploring the use of digital and social media, few are capitalising on the full potential of the technology and platforms.
A coordinated approach to using digital technologies should support and enable a wellbeing service to achieve its aims more effectively and efficiently. Digital can facilitate low cost ways to better engage with more residents and support them to make and sustain changes that benefit their health. For example digital channels can be:
- Used to engage with higher volumes of residents than traditional channels and in a more engaging and participative way.
- More effective at engaging with targeted populations. For example the power of social media to target (by geography and demographics as well as other means) is more accurate and cost effective than more traditional means of advertising.
Using technology also enables a service to free up capacity to use traditional methods to engage with residents for whom the digital approaches are not the most suitable. For example, automating some email and SMS communication can focus other resources on delivering face to face or over the phone interactions with those that need it.
Digital approaches can also:
- Facilitate deeper engagement and peer-to-peer interaction. For instance, a stop smoking online community facilitated by a specialist Facebook group would enable service users to continue to support and motivate each other during and upon completion of traditional support.
- Reach residents who would otherwise not be engaged.
The scope of digital in this context
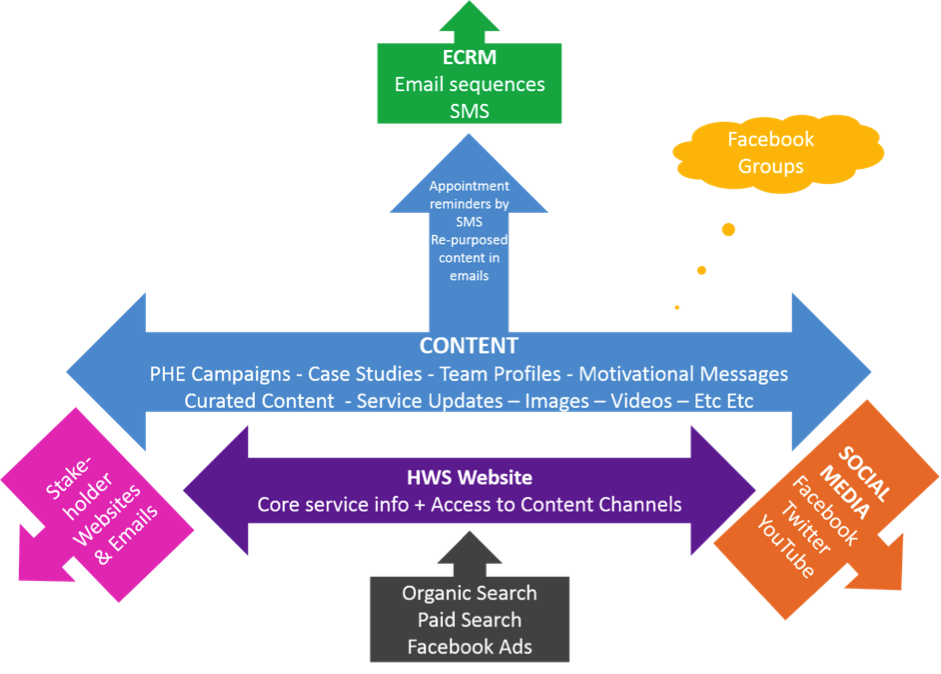
Having researched multiple wellbeing service providers, we have found that a best practice digital approach will generally consist of:
A. The Website
- Possibly incorporating a blog – ideally hosted independently from the local authority website and with two purposes:
- A point of contact for residents and service users for information, advice, online behavioural change tools, links to other service providers
- A data capture mechanism working in tandem with an eCRM system
- Websites should be responsive (i.e. mobile friendly)
- Websites should not be huge and cumbersome repeating detailed information found elsewhere, instead they should act as a portal pointing to external resources
B. Electronic customer relationship management (eCRM) system
- Builds a single view of service users but is shared across multiple services.
- Records all interactions with the service user (possibly including data inputted by health referrers) and facilitates tailored and timely electronic communications.
- Note there are data protection issues with this, particularly if servers are outside the EU (normally the case with the popular American systems).
C. Social media
- Used for recruiting new users and engaging with residents
- Social media facilitates peer to peer interactions
D. Apps and text messages
- Supporting residents to use online behaviour change tools such as those provided by PHE, the NHS and those being developed locally or by other third parties
- and facilitates tailored and timely electronic communications Use of digital communication channels such as emails and SMS (text messages) to recruit and continually engage residents. For example to reduce “did not attends” (DNA’s) for appointments, or to provide on-going motivation during a quit attempt, or to provide self-reported feedback after completion.
Use of digital platforms
Aims of digital
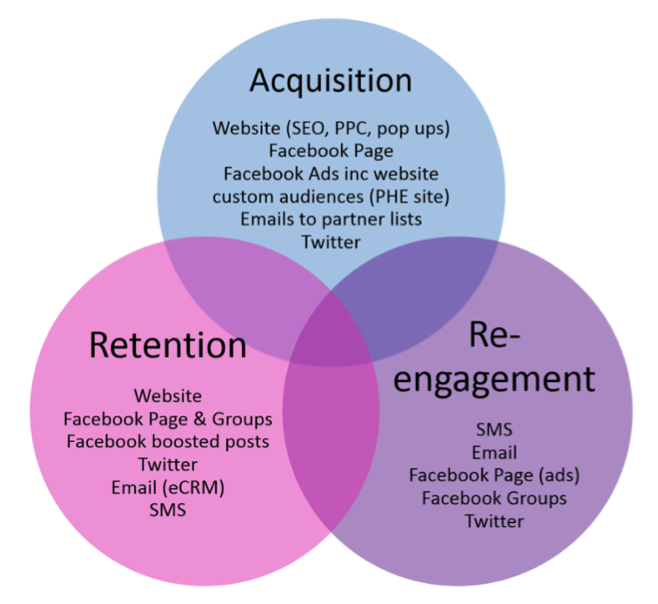
Service providers can use digital approaches to:
- Recruit new users
- Retain existing users
- Re-activate users
- Remotely motivate and support behaviour change attempts
- Monitor user engagement with communications
- Facilitate user engagement with other local services
- Present a “joined up” approach to communications and service provision
- Gather user feedback
Communication channels
A number of communications approaches are normally required to achieve these aims – for users there is no “one size fits all” approach. So for instance Facebook could be used to do the following:
- Recruit new users as a result of targeted advertising
- Re-activate users as a result of advertising targeted at a custom audience (using email addresses of lapsed users
- Retain existing users and enable their success via motivational and informative content on the website and social media presence
Example: In order to engage with a 35 year old male resident who wants to stop smoking the service could use social media, online advertising and traditional marketing methods to encourage residents to visit the service website. This multi-layered approach can often be more effective (or act as a tipping point) to enable self-referral.
- The resident may see a Twitter post about the Stoptober campaign, a Facebook ad, or see a poster on the high street.
- He may well later search Google for how to access Stoptober locally (and see a PPC ad).
- Once on the website he will be incentivised to provide his email address and phone number at first point of service access.
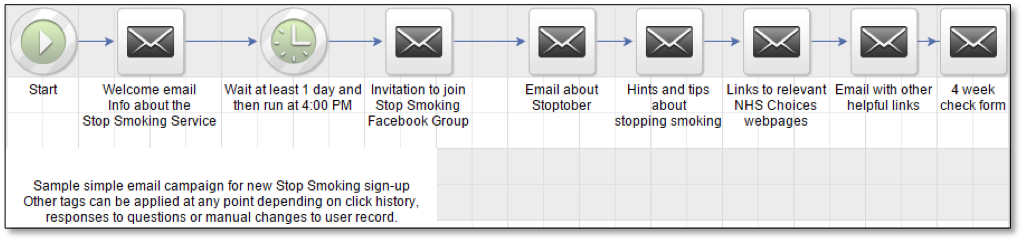
- This data would populate the eCRM system and trigger email sequences (see below image) such as a welcome email, and alert service providers to a potential user.
- The user may then be directed to try a relevant online behaviour change tool
- The user may also be prompted to sign up to attend a drop in session at a local venue. They would receive a reminder text message the day before the drop in session.
- When attending a drop in session the stop smoking advisor can access their details from the eCRM database and add in additional information such as a CO reading and quit date.
- Whilst making a quit attempt they could be invited to a specialist Facebook group for local quitters where they could interact with other residents, share stories and provide motivation. Successful quitters can become positive role models and continue to engage with new users.
- At 3 months and 12 months after quitting they are automatically send a text message, asking whether they are still smokefree. They reply with a text message that updates their record in the eCRM.
- Once they have been successful in making one lifestyle change such as stopping smoking, they could be offered support in other lifestyle areas following a similar process.
What is already available?
NHS Choices and Public Health England (PHE) produce an extensive set of resources that can be repurposed in communication channels. PHE produce an annual calendar of campaigns and activities that often receive national media exposure allowing local services to maximise their communications impact.
| Good practice guidelines from the NHSThe NHS paper Healthy Weight, Healthy Lives: Consumer Insight Summary provides excellent advice on messaging in relation to health promotion communications.Snippets include:“Parents don’t want to be lectured. They want empathetic messages from peers, not diktats handed down from the great and the good and from the government”.“Diet and activity messages need to be kept separate [otherwise the activity component is ignored]”“Direct references to ‘obesity’ and ‘weight’ alienate parents and may mean they fail to recognise themselves as part of the audience for a campaign or intervention”“Use ‘we’ rather than ‘us’ and ‘you’”“Use the kind of colloquial phrases that parents use themselves, like ‘bags of energy’”“Images of happy, healthy children draw parents in… images of very overweight or obese children also encourage deselection”Rather than repeat it all here, we advise to read and follow the advice on pages 65-71http://www.nhs.uk/Change4Life/supporter-resources/downloads/Consumer_insight.pdf |
Similarly material from other wellbeing services can be “borrowed” (we call this repurposing or curating content) (e.g. articles, tweets, links to “found” content). Many newspapers and specialist websites also produce well-written, relevant material that can be shared.
So whilst it is possible to create unique, original content (and this is clearly important for local service information), it is more cost effective to repurpose or point at third party resources.
Using technology for greater efficiency
Whilst requiring investment in set-up, technology can be utilised to automate processes. Electronic customer relationship management (eCRM) describes all forms of managing relationships with customers using digital technologies, for example some eCRM systems integrate your internal client database with a bulk emailing tool and SMS features. eCRM systems can be used to send a sequence of automated emails with helpful links, advice and motivational messages to people who have expressed an interest in stopping smoking or weight loss.
Approaches such as email and SMS rather than physical mailings should be employed to keep costs down. Such automation, once set up, minimises the need for repetitive staff input. It is also simple to monitor who has read which messages so triggering different future approaches dependent on exhibited behaviour.
Whilst automated digital communications can replace much human contact, it is still essential to humanise communications and show services are for ‘people like me’. This can be achieved by practices such as providing named contacts in emails, team photographs in “About Us” pages, profiles and interviews with staff and health champions, testimonials and stories from users.
This is part of our full report on how digital technology can be incorporated into Local Authority health and wellness services with the aims to save money, work smarter, increase referrals and help more people locally to improve their health. The report is essential reading for public sector professionals working on any form of marketing communications and digital service delivery within local authority teams and service providers. Click here to visit the report home page.
Next section
Social media channels >